
The microbes strike back
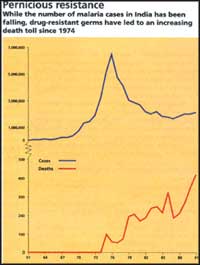 Malaria -- whose incidence dropped from an estimated annual 75 million cases with 0.8 million deaths before Independence to 0.1 million cases with no deaths by 1964 -- showed feverish activity in the '70s. It is stabilising now at about 2 million cases a year. Of late, however, a potentially fatal form of malaria, caused by Plasmodium falciparum, is accounting for as much as 35-40 per cent of the cases and is spreading to new areas.
Malaria -- whose incidence dropped from an estimated annual 75 million cases with 0.8 million deaths before Independence to 0.1 million cases with no deaths by 1964 -- showed feverish activity in the '70s. It is stabilising now at about 2 million cases a year. Of late, however, a potentially fatal form of malaria, caused by Plasmodium falciparum, is accounting for as much as 35-40 per cent of the cases and is spreading to new areas.
An uncommon strain of cholera, now coldly designated 0139 Bengal, broke out in Madras in October 1992, and spread to West Bengal and other Indian states and neighbouring South Asian countries. By December 1992, this strain accounted for 95 per cent of cholera cases in Calcutta, prior immunity and existing vaccines being ineffective against it. Says Jacob John of the Christian Medical College, Vellore, "The eighth pandemic of cholera has already started".
Tuberculosis afflicts 1.5 per cent of India's total population; the patients number 12.7 million, of which 3.4 million are infective. Every year, half a million Indians die of TB and 1 million cases are added. With the advent of AIDS, another 200,000 cases will be added annually by AD 2000, according to the World Health Organization (WHO).
Kala-azar, a severe systemic disease which, if untreated, proves fatal, had disappeared in India due to intensive DDT spraying under the malaria control programme in the '50s. It made a comeback in the '60s, wildly spread in 1977-78, and refuses to be subdued even now. There have been 250,000 cases (official figure: 77,101) in an epidemic outbreak in 1991, with the mortality rate ranging between 5-10 per cent, according to a report of the Tropical Disease Research (TDR) programme, jointly sponsored by the WHO, the World Bank and the United Nations Development Programme. It is still prevalent (official figure: 44,000 cases) and largely untreated in the endemic areas -- Bihar and parts of West Bengal -- with the pathogen, the microbe that causes the disease to slowly develop resistance to drugs.
THE microbes are striking back.
Suddenly, diseases that were ostensibly banished are now on the warpath. At the recent outbreak of what was supposed to be the plague, which showed up in India after 30 years of oblivion, former director general of the Indian Council of Medical Research (ICMR), V Ramalingaswami, made an ominous observation, "Infectious diseases are waiting in the wings to exhibit their re-emergence or enhanced virulence."
Like a doomsaying coming true, just a few weeks later, a virulent form of malaria hit 60,000 people in Rajasthan, killing many in an area that has never witnessed the disease (Down To Earth, Vol 3, No 13). A look at the country's health data reveals that the disease graph is running wild. There are many reasons behind this phenomenon: the first is "ecoiological" changes -- like the drug resistance of pathogens, the insecticide resistance of vectors (germ carriers), the emergence of new pathogen strains, environmental changes, and HIV-caused decreasing immunity in people. The 2nd reason, according to experts, is the human factor -- infrastructural inadequacies, administrative apathy, and policies that neglect the poor, who suffer the most. Shoestring budgets and lack of humanpower in rural public health centres compound the problem.
International agencies like the WHO foresee a rising occurrence of cholera, malaria, kala-azar and TB. According to Ramalingaswami, these diseases will piggyback along with Japanese encephalitis and dengue haemorrhagic fever, both spread by mosquitos and now sprouting up in various parts of India.
For a developing country like India, disease resurgence means a major addition to the country's already crippling medical burden. Take the case of TB: a 1992 WHO review report on the so-called Tuberculosis Programme in India noted, "The burden of tuberculosis in India is staggering. More than half the adult population is infected." The disease develops only in a small fraction of the population as the others have a natural immunity against it. But as the AIDS-causing HIV throttles the immunity level in people, the suppressed TB germs will go hog wild on more people. Further, resistance to antibiotics is estimated to be as high as 20 per cent in India, and will obviously add to the curative and preventive mess.
In the case of malaria and kala-azar, the resurgence was caused by complacency on the part of the state governments and health workers once they had curbed the diseases. Ramalingaswami points to instances of plague monitoring centres and rodent control cells being shuttered down once the disease apparently disappeared, and malaria eradication becoming rockbottom priority as the number of cases dwindled.
In India, says Ramalingaswami, this slippage on the part of the authorities began with malaria bouncing back 2 decades ago. "Then came the resurgence of kala-azar in the mid-'70s, after a point had been reached when there were no cases to demonstrate to medical students for years." Adds D Banerjee, professor emeritus, Centre for Social Medicine and Community Health, Jawaharlal Nehru University, New Delhi, "The resurgence of the diseases, like kala-azar in the '70s, took place as the information system and surveillance facilities set up by the post-Independence government became obsolete. No preventive action, therefore, could be taken on time."
A major, but often overlooked, eco-biological factor in disease resurgence is human-engineered environmental changes. For instance, the Indira Gandhi Canal in Rajasthan, and the waterlogging and flood irrigation it led to, has been blamed by field workers for the rise in malaria vector anopheles mosquitos in the area. Also, in development projects, migrant construction workers often play the role of disease carriers. The Bradford Morse committee review report of the Sardar Sarovar Project (SSP) for the World Bank noted analogically, "The ignition wire of construction-related stagnant water and the gunpowder of immigrant labour creates an explosion of malaria."
In India, malaria became a byproduct of the mega irrigation projects in Punjab, Haryana and Karnataka. Says the Morse report, "Malaria in Karnataka soared by a factor of over 250 due to Upper Krishna irrigation project." The SSP area, along with nearby villages, has "a high level of malaria with the killer type (P falciparum) exceeding 30 per cent," said studies for the World Bank done by public health expert N L Kalra. Since 1990, as the construction progressed, people started dying of malaria, Kalra pointed out to the Bank, which partially funded the project. The Morse report warns of "the likelihood of Japanese encephalitis in the coming 15 to 20 years".
Kala-azar (leishmaniasis) also has a developmental background, according to environmentalists. Waterlogging created by the river embankments built as flood control measures often provide ideal habitats to the vector sandfly (Phlebotomous argentipes). Says S Sehgal, director in-charge, National Institute of Communicable Diseases (NICD), Delhi, "Sandflies are very sensitive to environmental changes."
Unplanned urbanization
Noting that "the number of leishmaniasis cases has increased significantly during the last decade," the TDR lists the causes for the kala-azar resurgence: new settlements in rural areas, environmental changes, wars, and unplanned urbanisation.
In the case of TB, the congested, dirty ghettos of the poor in the South and the North have become the ideal breeding ground for Mycobacterium tuberculosis, which spreads through air. As has long been established, Vibrio cholerae spreads through ponds, lakes and groundwater aquifers contaminated by the excreta of disease carrying people. Urban slums breed the disease during the monsoons when the rains wash down excreta into the groundwater and the shallow handpumps pull up the gunk, as happened in Delhi in 1989.
Studies during the 1992 epidemic of non-01 cholera have reinforced the disease's environmental connection. Says S K Bhattacharya, deputy director, National Institute of Cholera and Enteric Diseases, Calcutta, about a study done at a 40-sq km lake in East Calcutta, "The highest isolation of V Cholerae 0139 in this study was made from surface waters indicating the gross contamination of the freshwater lake during the period of the 0139 epidemic in Calcutta." People used the lake water only for washing and bathing, but they still contracted infection as easily as the people who imbibed the contaminated water.
Bangladeshi scientists attribute the advent of the non-01 type cholera to environmental pollution. A K Siddique, head of the Epidemic Control Preparedness Programmes, Bangladesh, says that toxic industrial chemicals and fertiliser residues from the fields "may have induced adverse effects in V cholerae 01 and/or may have given selection advantage for the new strain."
The importance of clean surroundings is often brought to bear only when a disease breaks out. The pneumonic plague outbreak in Surat followed a major flood and accumulation of garbage. In Beed, the bubonic plague followed the earthquake in nearby Latur, which dislocated hordes of rodents. In both, the warnings of environmentalists and health experts to rectify the sanitary lapses had gone unheeded.
Says Ramalingaswami, "It is important to examine the relationship between population and local eco-systems and local environmental resources and consider the 'response elasticities'." The problem, as Ramalingaswami puts it, is that the government ignores the local environmental-human interaction while formulating its health policies.
A major hurdle in fighting diseases is the growing drug resistance among microbes; it is, in fact, a stumbling block in the worldwide battle against TB and malaria. In India, it has begun to block kala-azar treatment as well. Fortunately, the non-01 type cholera has so far responded to common drugs, though not to vaccines and prior immunisation. Developing resistance is, in fact, part of the parasite's natural fight for survival. However, incomplete treatment and indiscreet medication, which are unfortunately common, help enhance microbial drug resistance.
When the pathogens resist the 1st-line treatment -- the common initial drugs -- doctors resort to the 2nd-line, which is administering stronger, more expensive medicines, which also have more side-effects. The problem becomes acute in cases of multiple drug resistance among the pathogens. Says V P Sharma, director, Malaria Research Centre (MRC), Delhi, "There have been cases of malaria in Thailand that do not respond to any known anti-malarials." Meanwhile, multi-drug resistant TB, which has become a nightmare in the clinicalised West, has begun to be noticed in India, too.
The science of acquiring drug resistance is apparently simple. Explains J C Samantaray, a microbiologist at the All India Institute of Medical Sciences (AIIMS), "If drugs manage to kill only the weak or susceptible pathogens in the body, the hardier, resistant ones survive the drug." The process of natural selection over generations gives rise to drug-resistant microbe strains.
In the case of M tuberculosis, antibiotics since the '50s have toughened them; there has been no major new drug against the disease since the discovery of wonder drug rifampicin in the '60s. "Tropical diseases are not good business because people afflicted with them have no money," said Andre Nikitin, a senior product manager at Ciba-Giegy, a giant Swiss drug multinational, to Newsweek (May 17, 1993). "Most people with TB are so poor they either get drugs for free or they die," he added. When TB boomeranged in the '90s, it came as a shattering shock. The medic's quiver had no new arrows to fight back with.
Four main drugs are used to treat TB -- isoniazid, rifampicin, pyrazinamide and ethambutol. Says Ashok Rattan, a TB specialist at AIIMS, "A minimum of 2 of these drugs are used for TB treatment, one to stop the growth of the bacteria and the other to kill them. To ensure complete cure, 1 or 2 more drugs are also given." The usual 6-month regimen prescribed by WHO includes the above mentioned drugs in different combinations. The Tuberculosis Association of India (TBAI), a nodal organisation that coordinates NGO and government work in the National Tuberculosis Control programme, has recommended another "standard regimen" which may extend up to 1 year or more. (The common TB vaccine BCG can prevent the disease only in children.)
TB drug resistance shows a rising trend in India, going by independent reports, "although it is not the major issue here," says D R Nagpaul, a technical consultant with TBAI. "In India, 80 per cent of the cases respond to antibiotics, if the full course of medicines is taken." Sadly, arbitrary treatment by doctors as well as the dropping out of the patients midway make control measures meaningless, and promote drug resistance, say WHO experts. A 1992 WHO study notes, "The patient is permitted to stop chemotherapy when he has completed 80 per cent of his prescribed regimen."
A survey of 102 private doctors in Bombay, by M W Uplekar of the Foundation for Research in Community Health, Bombay, and D S Shephard of the Harvard School of Public Health, revealed that they had prescribed 80 different TB regimens, while there are only 6 standard regimens recommended by health agencies. "Resistance to drugs is the inevitable result of poor management of control programmes," says Rattan.
Lack of drugs
The non-continuation of medication is often due to shortages of drugs and humanpower in the country's primary health centres. Rifampicin has often been in short supply, says Nagpaul. "One full course costs Rs 2,000; and money has always been in short supply." Another major case for default, as pointed out by the WHO report, is the shortage of certain drugs in the national market, often due to low-profit margins.
With regard to malaria, what worries health professionals is the rampant spread of the potentially drug-resistant P falciparum, which used to be restricted to endemic areas of the northeast and the tribal belt in Orissa. This virulent disease can affect the internal organs, including the brain (which is why it goes by the name of cerebral malaria) can kill 2 to 3 out of 100 patients, whereas the common variety cased by P vivax limits its action to the bloodstream and is not normally lethal.
The common 1st-line treatment for malaria is chloroquine, a quinine derivative. Chloroquine is quite effective against P vivax and a majority of P falciparum cases. But falciparum strains started showing resistance to the drug in the '60s in the northeast. "Chloroquine resistance has spread to all endemic regions," noted the 1991-92 TDR Annual Report. But the problem does not stop there. Says Sharma, "Some of the malarial cases do not respond even to the 2nd-line treatment with sulphadoxine; then the only lifesaving measure is the administration of quinine, which involves side reactions ranging from dizziness to deafness."
V S Orlov, the malaria expert at the WHO South East Asia Regional Office (SEARO), New Delhi, cautions that quinine ineffectiveness is widely reported in Burma, and that if preventive measures are not taken soon, it will infiltrate into India through the northeastern states. Predicts Orlov, "In 5 years time, quinine resistance will develop in India."
In the case of malaria, too, inadequate drug management, often done without diagnosis, can lead to drug resistance. "Whenever malaria cases break out, the municipal authorities supply drugs without supervision or follow-up," says S Kame, a local pathologist formerly with AIIMS. According to a reference paper published by A V Kondrashin, senior regional advisor (malaria) to WHO, presumptive treatment involving only the common 1st-line drug chloroquine can promote drug resistance.
Drug-resistant microbes prolong the period of morbidity or the term of the disease, thus putting an additional burden on an already rickety healthcare system. Says Sharma, "While conventional treatment of malaria with chloroquine costs next to nothing, the cost of treating a case of falciparum malaria, which is often resistant to chloroquine, may go up to Rs 5,000."
In this scenario, there will soon be a pressing need for better remedies. Says Ramalingaswami, "We have reached a level, where we should start looking for more efficient alternatives." Chinese scientists have extracted a potent antimalarial substance called artemisinin from the quinghaosu (Artemisia annua) plant, an ancient remedy in China (see box: Historical ills), and 2 derivatives, artemether and artesunate, followed. According to TDR scientists, studies have indicated the efficacy of injective forms of these drugs (Down To Earth, Vol 3, No 2). Their molecular structure is different from quinine derivatives, which is why they might work even against resistant strains, Ramalingaswami argues.
In the case of kala-azar, drug resistance has led to use of stronger drugs with serious side-effects. The disease is caused by a protozoan parasite Leishmania donovani, carried by the female sandfly. For the treatment of kala-azar, the 1st-line drugs are antimony compounds, such as sodium antimony gluconate, developed over 40 years ago. The 2nd-line drugs are pentamidine, amphotericin B or allopurinol, all more toxic than antimonials. "Pentamidine causes diabetes and often you find several diabetic cases in villages hit by kala-azar," says C P Thakur, former head of the government-appointed Spot Assessment Committee on kala-azar. TDR programme scientists have stressed the need for safer and more effective drugs.
In the case of refractory patients, in whom the parasite tends to evade the drug, the disease relapses as Post Kala-azar Dermal Leishmaniasis (PKDL) after 2-3 years. In PKDL, the parasite leaves the usual target organs -- the liver and the spleen -- and enters the skin, forming nodules and protuberances.
Reliable data on drug resistance among kala-azar microbes is difficult to obtain because only about 1/5th of the total kala-azar cases are notified. Thakur, relying on field data, puts the rate of resistance against antimonials at 20 per cent. He points out that partial (FIGURES) drug resistance has been noticed in the treatment with pentamidine as well. But N B L Saxena, coordinator, Kala-azar Control Programme, National Malaria Eradication Programme (NMEP), maintains that very few patients show drug resistance -- about 7-8 per cent in all.
The financial burden of kala-azar can be staggering, the drug resistance adding to the expenses. The cost of 1st-line treatment is Rs 200-250, which covers one course of 20 injections; the complete treatment requires 4-5 courses, costing as much as Rs 1,500. The 2nd-line drugs are more expensive as they have to be imported. The treatment of PKDL would cost as much as Rs 15,000, Sharma notes.
In the case of new cholera strains -- non-01, specifically 0139, Bengal -- drug resistance is growing but is not yet as big a problem as with other diseases.
But the trouble with the 0139 strain is that the immune system of the human body fails to identify it. The first 6 recorded cholera pandemics since 1871 were probably caused by the "classical biotype" of V cholerae, whereas the 7th pandemic that began in 1961 was caused by a biotype designated ElTor. The 2 strains differ in a number of properties, including their virulence and the way they get attached to the intestine wall.
"The rapid spread of non 01 cholera is a cause of worry," says Bhattacharya. Within 6 months of its introduction in Madras, it spread to other South East Asian countries, Bangladesh being the worst hit. WHO reports show that 0139 has been isolated in 11 South East Asian nations, and imported cases were reported from USA, the UK and Germany. WHO has warned all countries in the region that they are "at risk" and stressed stronger surveillance.
In the case of malaria and kala-azar, the vectors have also evolved resistance to the insecticides used to exterminate them.